

Shouldn’t the after-effects of vaccination be discussed before?
MMR

Find out more about the MMR, and about the true nature of these childhood illnesses too. It’s not just a choice between MMR or obtaining single doses, which both have the potential to cause serious harm. After further research you may decide that contracting measles can play a beneficial role, resulting in priming and maturing your child’s immune system and increasing their well-being in adulthood – in which case you can say ‘No thank you’ to the MMR. There are numerous medical papers that indicate that measles and other childhood acute diseases lower the risk of developing conditions such as: brain tumours, cancers, leukemia and heart disease later in life. Why would we want to prevent that? What we do want to prevent is suppressing the illness resulting in secondary complications. This is mentioned further in the INTRODUCTION text box below.
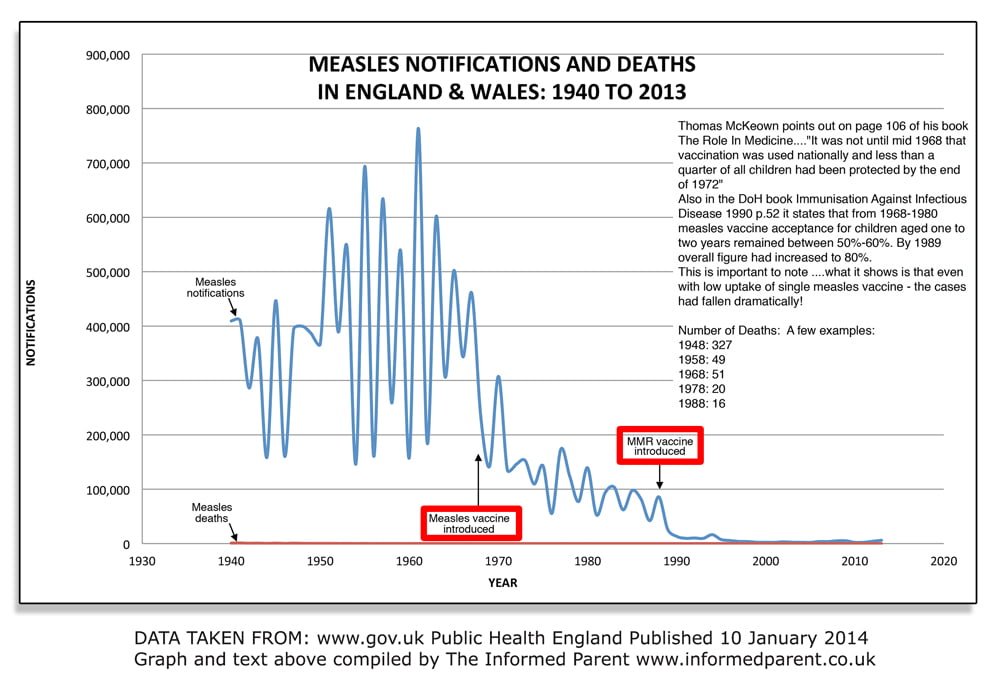
Thomas McKeown, author of the book ‘The Role in Medicine’ states:
‘With some variation in timing, the history of measles has been rather similar to that of whooping cough. The death rate fell continuously from about 1915; treatment (of secondary complications) has been possible since 1935; and mortality was at a low level before immunisation was used. It was not until mid 1968 that vaccination was used nationally and less than a quarter of all children had been protected by the end of 1972. I conclude that the contribution of immunisation to the reduction of notifications in the last decade cannot be decided on this evidence.’
Regarding recent media scaremongering coverage on measles outbreaks across Europe the EFVV website has a downloadable file with comments and data HERE
INTRODUCTION
INTRODUCTION
There is a vast amount of information on this subject and it would be impossible to cover all aspects.
This factsheet is to give you a starting point which I hope will prompt you to further research. I have focused predominantly on measles as this appears to be the one which parents have been made most anxious about. Further information on mumps and rubella will be added in due course.
Measles, mumps and rubella are generally straightforward acute childhood infections which most reasonably healthy children will sail through. No one is denying that in some rare situations some UK children will develop secondary complications but what we should be asking is why this should occur to those few? The message from the health department is that these diseases, especially measles, may strike your child out of the blue and may even be fatal.
Why would the measles virus randomly attack certain individuals and not others?
That is simply untrue.
Here are just a few things to consider:
• The level of health of the individual has an enormous influence on the outcome of a disease. Promoting one’s health is obviously the best way to reduce the risks of complications from any disease, and this can be primarily achieved by a good living conditions, clean water, sanitation, healthy diet, healthy lifestyle habits, exercise, emotional stability etc. •
• Mismanagement of the illness can play an enormous role in complications occurring. For example, parents are advised to give their baby or child fever suppressants at the first sign of a fever. Fever is the body’s response to sickness and suppressing this may lead to the disease being driven deeper into the system and possibly result into secondary complications.
• Overfeeding at the time of infections can also lengthen the time of recovery, children who are well-rested and kept on fluids at the initial stage of infection usually sail through these conditions much quicker.
• Benefits of childhood acute disease. Find out more about dealing with childhood infections, some holistic practitioners run courses for parents on these areas. Many holistic practitioners view illnesses, such as measles, as beneficial to the child, ie helping to prime and mature their immune systems and acting as a de-tox in childhood. This would then aid towards them becoming healthier adults. This has also been observed in medical studies, here are just a few examples:
Association of measles and mumps with cardiovascular disease: The Japan Collaborative Cohort (JACC) study
Kubota Y, Iso H, Tamakoshi A Aug 2015 Vol 241, Iss 2 p682-686
CONCLUSION: Measles and mumps, especially in case of both infections, were associated with lower risks of mortality from atherosclerotic CVD.
History of chickenpox in glioma risk: a report from the glioma international case–control study (GICC)
Amirian, Scheur, Zhou, Wrensch et al; Cancer Medicine 2016; 5(6):1352–1358
‘…we found that a positive history of chickenpox was associated with a 21% lower glioma risk, adjusting for age and sex’….Furthermore, the protective effect of chickenpox was stronger for high-grade gliomas.’ (gliomas = brain tumour.)
Cytotoxicity of glioblastoma cells mediated ex vivo by varicella- zoster virus-specific T cells
Caniff, Donson et al; J Neurovirol. 2011 October ; 17(5): 448–454. doi:10.1007/s13365-011-0048-z.
Do childhood diseases affect NHL and HL risk? A case-control study from northern and southern Italy.
Montella, Maso, Crispo et al; Leuk Res. 2006 Aug;30(8):917-22.
‘In addition, our study shows that measles may provide a protective effect against NHL.’ (non-Hodgkin lymphoma.)
Childhood infectious diseases and risk of leukaemia in an adult population
Parodi, Crosignani, Miligi, Nanni et al; Int. J. Cancer: 133, 1892–1899 (2013) VC 2013 UICC
‘Our results pointed out a protective role of childhood infectious diseases on the risk of CLL in adults.’
Mumps and ovarian cancer: modern interpretation of an historic association
Cramer, Vitonis, Pinheiro et al; 2010 Aug:21(8): 1193-201 PMID 20559706
Conclusion: Mumps paotitis may lead to expression and immune recognition of a tumor-associated form of MUC1 and create effective immune surveillance of ovarian cancer cells that express this form of MUC1.
Measles virus infection without rash in childhood is related to disease in adult life.
Ronne T; Lancet. 1985 Jan 5;1(8419):1-5
‘There was evidence of association between a negative history of measles, exposure in early life and development of immunoreactive diseases, sebaceous skin diseases, degenerative diseases of bone and cartilage, and certain tumours.’
——————————————-
VACCINATION STATUS
The vaccines given to babies in their first year, or indeed at any time may place a burden on the immune system so that the child is unable to produce a natural response to an acute illness, such as measles. This could also result in a more complicated case, however this appears to be another area that is rarely considered or studied.
It wasn’t that long ago when measles was viewed in a very different way, even by some medical practitioners, and parents would deliberately expose their children to the disease in the hope that they would get it! Why have parents become so scared of this disease now? Most parents are not too concerned when their children develop chickenpox, and yet the chickenpox vaccine has been introduced in a number of countries – as something every child should have, with the dangers of having chickenpox overstated.
When a new vaccine becomes available, in order to justify yet another vaccine in the programme, the possible complications of that disease are grossly exaggerated in order to create a fear. It also creates an instant demand for the vaccine! It is highly likely that the chickenpox vaccine will be introduced into the UK schedule at some point – in line with other parts of the world.
ALL vaccines, whether given as multiples or individually have the potential to cause various degrees of damage, from subtle to severe. Additionally, there are numerous published outbreaks of measles, mumps and rubella (world-wide) which have occurred in highly vaccinated populations. If you read about outbreaks but there is no indication as to whether they were vaccinated then it is highly likely they were VACCINATED – as unvaccinated case/cases developing measles would make headline news just to scare the public.
The choice whether your child receives the MMR, single vaccines (privately) or none at all is entirely YOURS, so don’t be pressurised into going ahead with them if you are not entirely sure. It is for YOU to decide, so give yourself all the time you need, these vaccines can be given to adults so you do not have to decide by the time your baby is 12 months old.
SINGLE MEASLES VACCINE AVAILABILITY
Regarding obtaining the vaccines separately – a brief history:
In the Dept of Health handbook, 1996, it stated: ‘Single antigen measles, mumps and rubella vaccines are available.’ However this changed back in the late 1990s. Why? Pasteur Merieux, the producer of the single measles vaccine ceased to supply Britain with this vaccine (1999). The two main reasons they gave were, firstly they could not meet the demand, and secondly, as they could not offer the complete trio as single vaccines, they felt it would be ‘unethical’. If the government were to give their mumps vaccine a license, then the company would reconsider.
It’s interesting to note that back in March 1998 (Evening Standard, 4/3/98) Pasteur Merieux indicated that they would be willing to create extra doses of single measles vaccine if the DoH specifically ordered it, despite not being able to offer single mumps vaccine. (No ‘unethical’ concerns raised then?)
The official line is that the MMR is ‘safe and effective’ and the DoH does not wish to encourage parents to obtain single vaccines. At present parents have to choose between MMR or nothing, unless you can find a private clinic offering single doses. Also be aware that due to the lack of safety studies and long-term follow up studies it is not clear that single vaccines are any less damaging than the MMR.
A word of advice – if you do decide to proceed with single vaccines, or indeed with the MMR please ask the doctor/nurse administering the vaccine/s if they will sign to take full responsibility should any kind of reaction occur. Also ask for details of the brand and batch number of the vaccine used – to keep for future reference in case of any reactions, as sensitive information on medical records does sometimes go missing.
Some parents are turning to other forms of medicine, such as homeopathy, osteopathy, naturopathy etc to treat their families. You can usually obtain lists of qualified practitioners in your locality from the various organisations.
I hope some of the points raised here in the introduction, and the following text, will be helpful towards enabling you to make an informed choice based on facts rather than scaremongering statements from health officials.
MEASLES
MEASLES
Measles is a viral disease. It is believed to be contagious for 7 or 8 days, beginning 3 to 4 days before the rash appears. ‘No treatment is required other than bed rest, plenty of fluids to combat possible dehydration from fever, and calamine lotion or cornstarch baths to relieve itching.’ (Taken from: How to raise a healthy child… By Dr R Mendelsohn.)
In the UK deaths from measles had declined by 95% BEFORE the measles vaccine was introduced in 1968. This decline was mostly due to better public health measures i.e. clean water, sanitation, improved living conditions, better nutrition.
Measles cases had been declining during the first half of the 20th century – well before the measles vaccine was used. When the vaccine was introduced the uptake ranged only between 30-60% in the years 1968-80 and yet measles cases continued to decline despite this fairly low uptake. Why? – because measles cases and the severity were declining anyway.
MMR vaccine was introduced into the UK schedule in 1988.
In 1964, before introduction of measles vaccine in 1968, deaths were recorded at 1/5,000 notifications.(1) By 1983 measles deaths were still recorded at 1/5,000 with a vaccine uptake rate of 50%.(2)
France, by comparison, also licensed measles vaccine in 1968 but had an uptake rate in 1983 of less than 20%, and experienced a measles death rate of 0.56/million. (3) Thus, after 15 years of using the measles vaccine in the UK, the danger from measles, which had declined for more than 50 years, was apparently unchanged, whilst in France, with little use of the vaccine, measles continued to become less severe.
The DoH still quote measles complication rates at 1/15 (4) which is the same rate reported in a study from 1964.(5) In that study respiratory problems and otitis media (middle ear infection) accounted for most of the complications.
Discussing measles deaths, The Lancet (1/8/81 p236) says: “In the UK about 1% of people with measles are admitted to hospital, and 1 in 10,000 may die….children who die from measles are typically those with malnutrition, or some other severe inter current condition, who would soon die from some other cause if not from measles…..Half of the 132 deaths attributed to measles in the first 6 months of 1961 were in children with serious chronic disease or disability.”(6)
And yet on the NHS website (August 2017) under measles complications it states: ‘It’s estimated around 1 in every 5,000 people with measles will die as a result of the infection.’ This figure is very misleading – let’s look at some data.

On the National Archives website, for example, when adding all the notification totals for the years from 2000 – 2012 the total number of measles notifications equates to 41,262.
Based on the NHS estimated figure you would expect 8 deaths from 41,262 measles cases. Between 2000 and 2012 there were actually 2 deaths from measles.
2006: A 13 year old male who had an underlying lung condition and was taking
immunosuppressive drugs.
2008: A 17 year old male – Public Health England describe the case as in an unvaccinated child.
(He was in fact born with a congenital immuno-deficiency and could not be vaccinated.)
SSPE
: Subacute sclerosing pan encephalitis
This condition is highlighted to frighten parents about measles infection even though it is a VERY RARE complication of measles that generally occurs 7 years after natural infection or 3.3 years after measles vaccination.(7) The rate of SSPE in the UK is calculated at 4/100,000 cases of measles and 1.4/million doses of vaccine.(8) The rate in France by 1983 at 1/2.6 million is even less than the risk from the vaccine.(9) SSPE appears to be caused by a reduced immune response to measles (10) with most affected children having a history of measles infection in the first years of life or exposure to live measles vaccine. (11)
PANORAMA & THE CASE OF ADAM MORRISH
The Private Eye ‘MMR Special’ May 2002 reported:
‘In February 2002 the BBC’s Panorama told the tragic story of 21-year-old Adam Morrish, who was slowly dying from SSPE (subacute sclerosing panencephalitis) —a degenerative condition similar to vCJD but caused by the measles virus attacking the brain.
In Panorama’s investigation of the MMR/autism controversy, Adam’s plight provided a powerful reason for having the jab. The programme said he had been exposed to measles after sitting near an unvaccinated child on a bus. Curiously, it did not say if Adam had been ever been vaccinated or not, which may have played a role in this tragic case.
In fact Adam did receive an MMR booster some two to three years before he began to develop SSPE shortly before his 12th birthday. However, he had been exposed to natural wild measles in 1982 when he was only 15 months old, before vaccination. Panorama said that because the usual progress of SSPE takes several years, it was much more probable that his fatal infection was caused by the wild measles he suffered as a toddler, rather than by the vaccine he received later.
The programme makers said they and the Morrish family decided not to reveal that Adam had had MMR because it would “confuse” the issue. Although vaccine manufacturers have said SSPE has been recorded as an extremely rare adverse event, and the Vaccine Damage Payment Unit has paid out for vaccine-induced SSPE, the government now says it will no longer do so. This is because brain biopsy studies of 11 children in the UK who suffered SSPE all revealed wild strain measles — even in five vaccinated children with no history of exposure to wild measles. The health department suggests those children must have had a sub-clinical exposure to natural measles before vaccination. But the numbers on which this is based are very small.
What is known is that SSPE is very rare— some studies have put it at between or in 100,000 and one in a million. A study by a team of researchers in Ankara, Turkey, published in the medical journal Paediatrics looked at the histories of 350 victims of the disease, some vaccinated, some not. It found the onset of SSPE symptoms following exposure to natural measles was seven years while after vaccination it was three-and-half years — a time span very similar to Adam’s without biopsies, however, no one can say for sure what the trigger was in the Turkish cases or indeed in Adam Morrish’s case.’
The Informed Parent contacted one of the Panarama team, Sarah Barclay, regarding the fact that Adam Morrish had been vaccinated. Also a copy of the Paediatrics (7) article mentioned above was faxed to them. I was told that the team did not include this information in the programme as they did not think it was relevant.
MEASLES IN INFANCY IS A PROBLEM THAT HAS INCREASED
Women with vaccine-induced immunity have low levels of antibody to transfer across the placenta and consequently have babies who start life with low levels of antibody which may make them susceptible to infection at very young ages when measles can be more dangerous.(12) Testing of measles immunity in infants born to vaccinated mothers showed no immunity at 6 months of age in 93%, whereas antibodies transferred at birth from mother to child normally remain present for 1 year.(13) Measles antibodies are lower in women young enough to have been vaccinated than in older women and only 2% of children born to vaccinated mothers have been found to be protected up to 12 months of age.(14) Please note that the role any level of antibody plays as regards to ‘immunity’ is also questionable.
Measles (and mumps) infection in vaccinated adolescents and young adults has increased since the use of both measles and MMR vaccines. Due to the uncertainty of what long-lasting ‘immunity’ is achieved in vaccine recipients this then leaves the possibility of pregnant women and other adults becoming susceptible to measles and mumps, at an age when complications are more likely to occur. Certainly, before the introduction of the measles vaccine, the universality of measles in childhood rendered adult infection a rare event.(15) Measles during pregnancy may result in low-birthweight infants, miscarriage, premature labour and possibly fetal abnormalities.(16)
During the 1980s measles increased dramatically in the US especially in secondary school populations with 30 -100% of measles cases in vaccinated children. “The apparent paradox is that as measles immunisation rates rise to high levels in a population, measles becomes a disease of immunised persons.”(17) As a result a 2-dose schedule was introduced but the long-term effect of the 2-dose strategy (given at 15 months and 4-6 or 10-12 years) “remains to be determined.”(18)
In the 1994 measles/rubella vaccine campaign in England and Wales, the Dept of Health acknowledged that 10% of vaccinated children do not have measles antibodies.(19) This 10% are classed as primary vaccine failures, i.e. they develop no antibodies after vaccination, thus the vaccine is considered to be 90% effective. However, secondary vaccine failures also occur, that is, an initial production of antibodies after vaccination that decline to low levels and allows re-infection. The rates of secondary vaccine failure are unknown but it is accepted that antibodies are an indicator of immunity and not proof,(20) in other words antibody production after vaccination does not equal immunity.
Since November 1994, following on from the measles/rubella vaccine campaign, laboratory confirmation by testing salivary samples has been required for all clinically diagnosed measles cases.(21) Apparently the existing national surveillance system for measles, which relied on clinically diagnosed cases, lacked “the precision required for effective disease control”, whilst, at the same time, other viruses causing measles-like illness need to be looked into.(22)
According to the salivary test, which is extremely sensitive, measles is now wrongly diagnosed in 97% of cases report the Public Health Laboratory Service who note that it is “inherently difficult to make a diagnosis based on clinical symptoms alone. Any doctor would find it difficult to differentiate between viruses.”(23)
WELL-MANAGED MEASLES IN HEALTHY CHILDREN – A ‘HEALTHY’ OPTION?
Epidemiological studies have led to speculation that infections in early childhood may prevent allergic sensitisation. In Guinea-Bissau children who developed natural measles were found to be less atopic (allergic) than children who received the measles vaccine and had not had measles.(24)
An association has also been found between a negative history of measles rash in childhood with the development of immuno-reactive diseases, sebaceous skin disease, degenerative diseases of bone and cartilage, and certain tumours in adulthood.(25)
Immunological theory also indicates that infection can prevent allergy. A Danish paper asks whether we have to choose between measles or an increase in allergic disease? And if so, who should decide – the individual or society?(26)
Remission of atopic dermatitis after natural measles has been reported (27) as has measles-induced remission of psoriasis.(28)
Temporary remission of juvenile rheumatoid arthritis;(29) chronic idiopathic thrombocytopenic purpura; (30) hyperimmunoglobulin E syndrome;(31) and nephrotic syndrome (32) have all been reported after natural measles infection.
VITAMIN A & MEASLES
A great many studies have since shown that vitamin A supplements reduce the severity of measles. Vitamin A plays a central role in immunity and resistance to infection whilst a deficiency is associated with increased illness and death from infectious diseases; high-dose vitamin A supplementation reduces deaths in children with acute complicated measles by 50% and has reduced illness and death even among children with no symptoms of vitamin A deficiency;(33) Deaths from respiratory complications in measles can be reduced by 70%.(34) Vitamin A deficiency is also associated with otitis media as well as acute measles, even subclinical (symptomless) vitamin A deficiency is associated with increased illness and death.(35)
Most of the research into vitamin A and measles has been done in developing countries but vitamin A deficiency in its subclinical form is now a world health problem in young children and the problem in developed countries is probably under-recognised.(36)
In New York City in 1992, even children with marginally low levels of vitamin A (i.e. previously healthy) were more likely to have measles with: high fever; fever lasting 7 days or more; and to be hospitalised.(37)
In another study of American children with measles, otitis media occurred in those with low levels of vitamin A , whilst children with the lowest vitamin A levels had pneumonia or were hospitalised.(38)
Studies in English children seem to be confined to one published in 1932 when children with severe measles were given cod-liver oil (a good source of vitamin A) which resulted in a reduction in deaths of 58%.(39)
Department of Health in its literature to parents mention that, prior to 1988, more than half the acute measles deaths occurred in previously healthy children. However, as subclinical vitamin A deficiency has no symptoms and children with acute measles are not routinely monitored for vitamin A deficiency in the UK, it is difficult to know the level of this deficiency amongst UK children. Additionally, how many of these ‘previously healthy children’ were vaccinated with other vaccines that may have had an impact on how they dealt with a case of measles?
REFERENCES
1. Miller DL. Frequency of complications of measles. BMJ 1964;2:75-78
2. Miller CL. Current impact of measles in the UK. Rev Infect Dis 1983;5:427-38
3. Rey M, Celeres J, Mouton Y & Netter R, Impact of measles in France. Rev Infect Dis 1983;5:433-438
4. Immunisation against Infectious Disease. HMSO 1996
5. Miller DL. Frequency of complications of measles. BMJ 1964;2:75-78
6. Vaccination-The Hidden Facts by Ian Sinclair, p93 (The Lancet. Vol 318, Issue 8240, 1 Aug 1981, p236-7 : Rationalising Measles Vaccination.)
7. Modlin JF, Jabber JT, et al. Epidemiological studies of measles, measles vaccine and SSPE. Pediatrics 1977;59:505
8. Miller C, Farrington DP, et al. The epidemiology of SSPE in England and Wales 1970-1989
9. Int J Epidemiol 1992;21:998-1006
9. Rey M, Celeres J, Mouton Y & Netter R, Impact of measles in France. Rev Infect Dis 1983;5:433-438
10. Wechsler SL, Weiner HL, Fields BN. Immune response in SSPE: reduced antibody response to the matrix protein of measles virus. J Immunol 1979:123:884
11. J Pediatr Nurs 1991;6:87
12. The Lancet 1995;345:272
13. New Scientist 1989; Nov 4 :26
14. J Ped 1986;108:671
15. Clin Perinatol 1988;15:259
16. Arch Intern Med 1994;154:1815
17. Arch Intern Med 1994;154:1815
18. Arch Intern Med 1994;154:1815
19. Measles /Rubella Information for health professionals. Dept of Health 1994
20. Ped Infect Dis J 1987;6:848
21. CDR Review 1994;4:R141
22. BMJ 1994;308:1015
23. Pulse 1997; Jan 18 :36
24. The Lancet 1996;247:1792
25. The Lancet 1985;1:1
26. Tidsskr Nor Laegeforen 1997;117:688 29. Clin Exp Allergy 1993;23:44
27. Clin Exp Allergy 1993;23:44
28. Ann Trop Paediatr 1986;6:293
29. Acta Paediatr Scand 1981;70:419
30. J Clin Immunol 1988;Vol 8;Iss 3:207
31. Ped Res 1986;20:685
32. Nephron 1986;42:110
33. Clinical Infectious Diseases 1994;19:489
34. BMJ 1993;306:366
35. Clinical Infectious Diseases 1994;19:489
36. Pediatr Nurs 1996;22:377
37. AJDC 1992;146:182
38. Pediatrics 1993;91:1176
39. BMJ 1932;2:708
MMR - A GLANCE BACK TO 1990s
In Japan the MMR was introduced in April 1989. Immediately after, asceptic meningitis began to be reported. The following summary shows the governments announcements up until the withdrawal in April 1993.
10/09/89 – Incidence of meningitis 1/100,000-200,000 – MMR declared safe.
25/10/89 – Incidence of meningitis 1/30,000 – Government announce caution.
20/12/89 – Incidence of meningitis 1/a few thousand – Government announce only if parents want it.
31/05/91 – Incidence of meningitis 1/1200 – Government announce – needs parent’s consent.
30/04/93 – MMR ceased.
A letter was sent to the Ministry of Health and Welfare in Japan on 24th March 1998 to clarify the situation.
The questions asked were:
1. Why Japan dropped the MMR vaccine?
2. What alternatives are offered to protect babies from measles, mumps and rubella?
3. Would Japan ever reconsider introducing MMR?
The response, 2/4/98:
1. After the use of the MMR vaccine, after the vaccinations had been done, there were frequent reports of cases of non-bacterial meningitis.
2. We are using the individual vaccines.
3. At present there are no plans to re-introduce MMR
A ban that remains to this day as the agency awaits the development of a combined vaccine they consider safer. (https://healthytokyo.com/blog/mmr-vaccine-in-japan/)
• MEASLES/RUBELLA SCHOOL CAMPAIGN – 1994
In 1994 a massive MR school campaign was implemented targeting 5 – 16 year olds with a measles/rubella vaccine. This was due to the DoH stating that there was a threat of a measles epidemic. However there were concerns from some that this ‘so-called’ epidemic was an assumption based on a highly questionable mathematical model.
Dr Richard Nicholson, editor of the Bulletin of Medical Ethics called for an inquiry.
His main criticisms were:
1. There was never going to be a measles epidemic in 1995;
2. There was no justification for concomitant rubella immunisation;
3. The mass campaign was planned as an experimental alternative to a 2-dose schedule of measles, mumps and rubella immunisations;
4. The government knowingly misled parents about the need for the campaign and about the relative risks of measles and measles immunisation;
5. The Dept. of Health broke the European Union’s laws on contracts and tendering to ensure that specific pharmaceutical companies were awarded the contract to provide the campaign vaccines.
(These companies happened to have a vast quantity of MR vaccine which was just about to go past its sell-by-date.)
Also interesting to note that during the summer of 1994 in the BMJ: ‘Measles still occurs in schoolchildren despite the success of the vaccination policy. Two small outbreaks, affecting 30 children in a Cumbrian secondary school and 24 in two junior schools in Trafford, are reported in “CDR Review” (1994;4:R70-3, R73-5). Debate continues over the feasibility of a national campaign to vaccinate all schoolchildren. The high rate of vaccination with measles, mumps, and rubella vaccine now being achieved, however, makes it likely that even limited outbreaks will become increasingly rare.’ (BMJ 1994;309:68 July 2nd)
Despite the indication of ‘limited outbreaks’ becoming ‘increasingly rare’ published in July 1994, by September parents were being told of the threat of a measles epidemic with the possibility of deaths!
At that time parents were also told that even if their child had actually had measles infection that having the MR would not do them any harm. I was invited onto a programme on BBC Radio 5 Live along with immunisation co-ordinator, Dr Robert Aston. One caller phoned in and asked Dr Aston if it was safe to allow her child to receive the MR at school as she had only recently received a dose of MMR, around 6 weeks before. Dr Aston stated that it was perfectly safe even if given within the same week of the first dose. The presenter actually queried Dr Aston in a surprised manner ‘in the same week?’ and he restated his comment despite looking rather uncertain. Unfortunately I did not get the chance to challenge Dr Aston’s statement as I know that there are NO safety studies demonstrating that. Sadly doctors often make similar sweeping statements about vaccines that go unchallenged on these kind of radio/TV programmes, resulting in the public being misinformed further.
• MEASLES OUTBREAK IN IRELAND – 2000
In the year 2000 there were just over 1500 cases of measles in Ireland, and this was used to create fear about the potential situation in the UK at that time.
‘Fears grow of measles epidemic in London’ – this was one of the headlines featured in The Independent, 27/11/00 by the health editor Jeremy Laurance. The article basically presented a scare-mongering scenario that ‘a measles epidemic could strike at any time because of the low level of immunisation among children in the capital.’
Dr Mary Ramsey, of the Public Health Laboratory Service stated that: “From the data available at the moment, several parts of London are already at risk of an epidemic. They have levels of immunisation low enough to be capable of sustaining an epidemic if the virus were introduced into the population.”
There was reference to a measles epidemic in Dublin which occurred over the year (2000), allegedly because of low levels of immunisation. The Informed Parent contacted the Public Health Laboratory Service for details of the measles cases in Ireland, and also the Eastern Health Board, Dublin (Mary Cronin). Based on the Irish figures supplied at that time on MMR uptake and notifications during the year 2000 the uptake was actually higher than other years. (See table below)

2 deaths in Ireland: These deaths were mentioned a number of times in the UK media, naturally frightening many parents about the measles. Unfortunately there were not any details included about why these two cases of measles would have resulted in death.
However, one journalist, Peter Hitchens, for the Mail on Sunday on 28/1/01 reported on the details of these two deaths in Ireland, stating:
‘One of the victims was a 12 month old baby girl from a very poor family living in grim conditions on a large Dublin housing estate and was, incredibly for a European capital in the year 2000, malnourished. The other was also exceptional and seriously ill before he contracted measles. He was a two-year old with a severe malformation of the throat which linked his windpipe with his oesophagus and who had to be fed by a tube into his stomach.’
• MMR SHOULD NOT HAVE BEEN LICENSED
Taken from: Sunday Herald, On-line edition, 11 December 2000
The controversial vaccine for measles, mumps and rubella (MMR) should never have been licensed, according to a shocking new report to be published next month. Senior clinicians, including a former medicines regulator at the Dept. of Health (DoH), argue that the MMR should not have been licensed in 1988 because there was insufficient evidence of its safety and the decision to license it was “premature.”
The leading authorities in the regulation of medicine are writing in the next issue of the Journal of Adverse Drug Reaction. They review a paper by Dr Andrew Wakefield, a consultant gastroenterologist at the Royal Free Hospital in London, and Dr Scott Montgomery an epidemiologist at Karolinska Hospital in Stockholm, on the process which led up to the introduction of the vaccine which has been linked to autism in children. Both are critical of the level of evidence supporting the introduction
of the jab.
Dr Peter Fletcher, who was a senior professional medical officer for the DoH in the early 1980s, also criticises the decision taken by his successors. In his review, which will be published in the journal, he says:
“Being extremely generous, evidence on safety was very thin, being realistic there were too few patients followed-up for sufficient time. Three weeks is not enough, neither is four weeks.
“On the basis that effective monovalent vaccines were available, the Committee on the Safety of Medicines (CSM) could be confident that delay in granting a licence would not result in a catastrophic epidemic of measles, mumps and rubella. Caution should have ruled the day, answers to some important questions should have been demanded and encouragement should have been given to conduct a 12-month observational study on 10-15,000 patients and a prospective monitoring programme set up with a computerised primary care database. The granting of a product licence was definitely premature.”
Another of the reviewers, Prof. Duncan Vere, a clinical pharmacologist and former member of the CSM, agrees that the observation periods for the tests of MMR were too short. “In almost every case, observation periods were too short to include the time of onset of delayed neurological or other adverse events,” he said. “Interaction between vaccines had not been considered adequately in children with multiple vaccinations and potentially ill-developed immune systems. He adds: “It is possible that a group of children exists who are developing a disorder with gastro-enteritis, abnormal reactions to measles virus and neurological disease. In the present condition they are highly likely to be vaccinated. The existing data throws no light on the question and new comparative studies are needed to seek an answer to it.” A note on the paper, which has been seen by the Sunday Herald, says: “In view of the serious implications of this paper by Wakefield and Montgomery, it was sent to a number of referees who have agreed to the comments they made on this paper being published. “These referees include the former chair of the medicines commission, a former member of the CSM, and a former principal medical officer in medicines division – now the Medicines Control Agency – of the DoH who served as medical assessor to the CSM.” Dr Montgomery, who formerly worked with Dr Wakefield at the Royal Free Hospital in London, said that the opinions of the reviewers were particularly interesting due to their background in the licensing of medicines. He said: “The people who reviewed this paper used to be in charge of drug safety and what they are saying is: “Should this vaccine have been licensed?” Nobody from the Journal of Adverse Drug Reactions can officially comment on the paper ahead of its publication next month, but a source from the journal said: “All reviewers conclude that something needs to be done about MMR and that there is a case to answer against the vaccine. “The first thing this paper says is that the MMR vaccine should not have been licensed. There was not enough evidence of the safety to license it. The view is that the evidence is inadequate.”
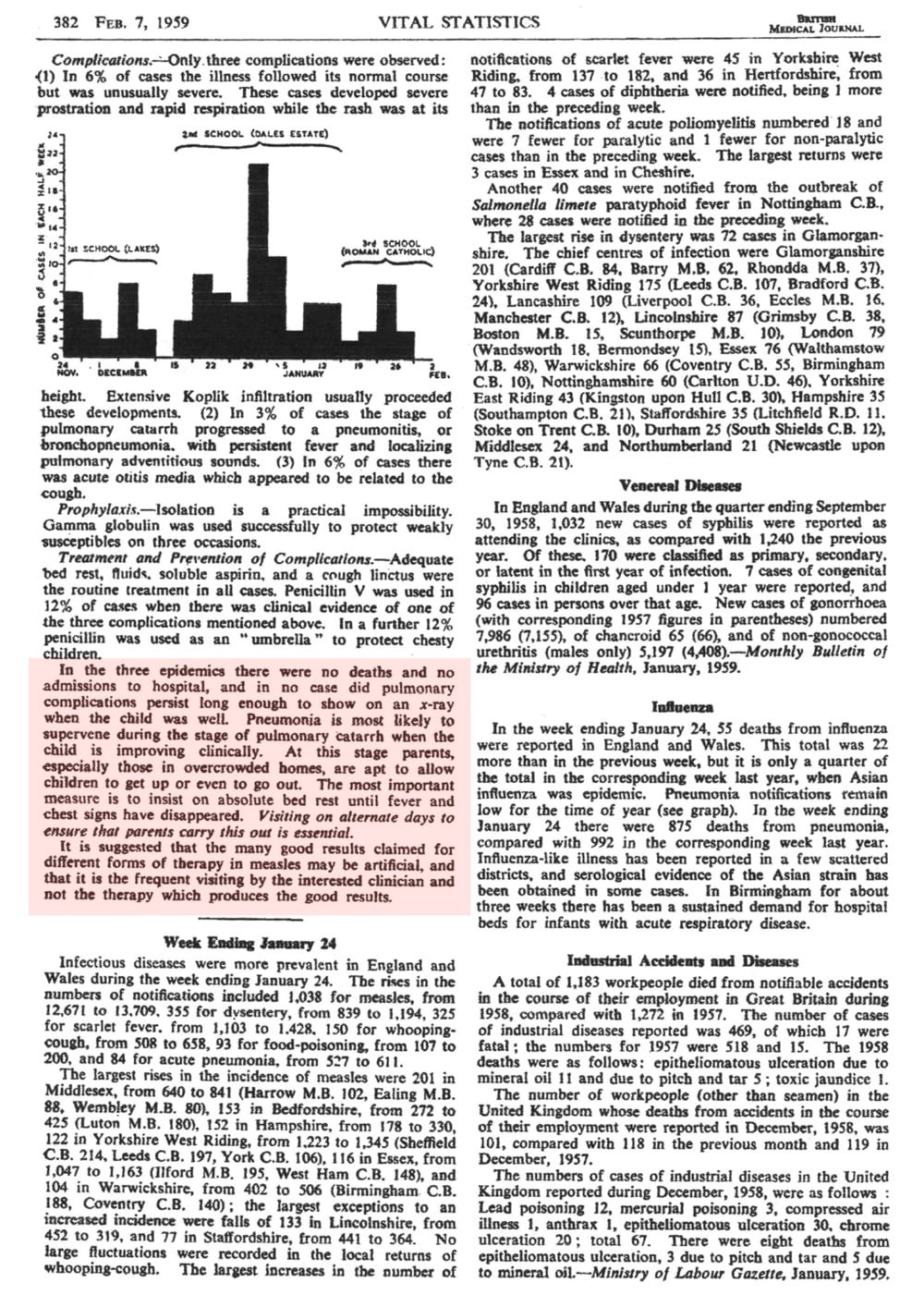
MEASLES WAS JUST A CHILDHOOD ILLNESS A FEW DECADES AGO!
Well worth reading – in terms of how measles was viewed over 60 years ago!
I have copied the text and pasted in for easier reading.

1959 BMJ
Also in the same publication – a few reports by GPs on measles outbreaks. (Three pages)
I have highlighted a few areas of text that make particularly interesting reading!
Notice how they are describing the cases…..very different to the description parents of today are led to believe. Also note that the adult cases were more severe – and yet since MMR we are seeing the age of incidence move to teenagers and young adults – not a very good achievement!


1962 GETTING MARRIED
Published my the British Medical Association.

1968 BMJ • VACCINATION FOR MEASLES

MEASLES IS VERY CATCHING!

SUSPECTED ADVERSE VACCINE REACTION?
The views expressed on this website and in the newsletter are not necessarily those of The Informed Parent Co. Ltd. We are simply bringing these various viewpoints to your attention. We neither recommend nor advise against vaccination. This organisation is non-profit making.